Why Clinical Case Discussion Improves Diagnostic Thinking for Medical Students

A clinical case opens in front of you.
You start thinking through it the way many medical students approach clinical cases during clinical case discussions or individual practice.A short history appears. A few symptoms stand out. Within seconds, a likely diagnosis forms in your mind.
As you read the rest of the case, you begin scanning for details that confirm that first impression.
The answer appears at the end. It matches. You move on to the next case.
If you have studied medicine for any length of time, this pattern probably feels familiar. Much of medical training encourages students to work through cases this way through textbooks, question banks, and exam preparation, often thinking through each scenario individually.
But clinical reasoning rarely develops in isolation.
When cases are discussed with others, the experience changes. Someone notices a detail you missed. Another student suggests a different differential diagnosis. A simple question forces everyone to reconsider the initial assumption.
Suddenly the case is no longer just about finding the correct answer. It becomes an exploration of how different clinicians think through the same clinical problem.
Over time, these conversations show why clinical case discussion plays an important role in developing diagnostic thinking during medical training.
Why Clinical Case Discussion Matters in Medical Training
Much of medical education trains students to solve clinical problems individually.
A case appears in a textbook, a question bank presents a scenario, or an exam asks for the most likely diagnosis. The student reads the symptoms, considers possible causes, and chooses an answer.
This process helps build foundational knowledge. But it often happens in isolation.
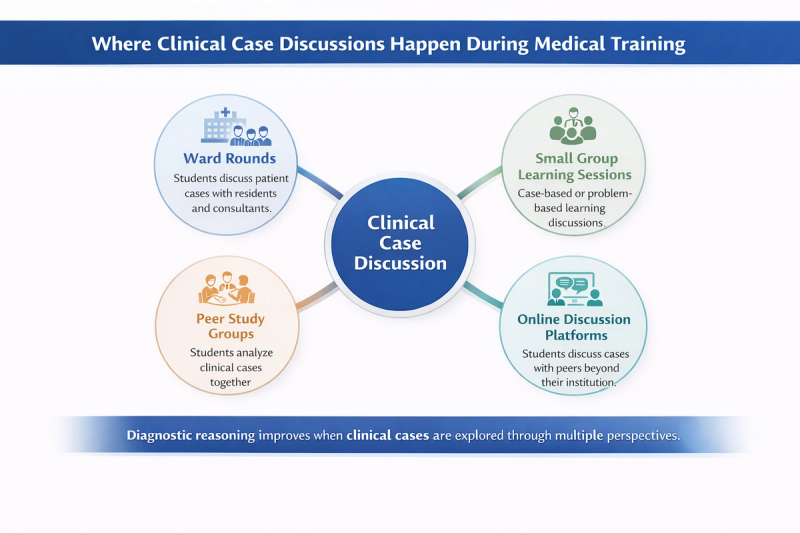
Clinical reasoning in real medicine rarely works that way. Diagnosis develops through conversations, questions, and shared interpretation of patient information. Ward rounds, case presentations, and multidisciplinary meetings all rely on discussion.
When diagnostic thinking becomes visible and discussable, students begin to understand not only what the correct diagnosis is, but how different clinicians reason their way toward it. This shift from individual answering to collaborative reasoning is one reason clinical case discussion plays an important role in developing diagnostic thinking during medical training.
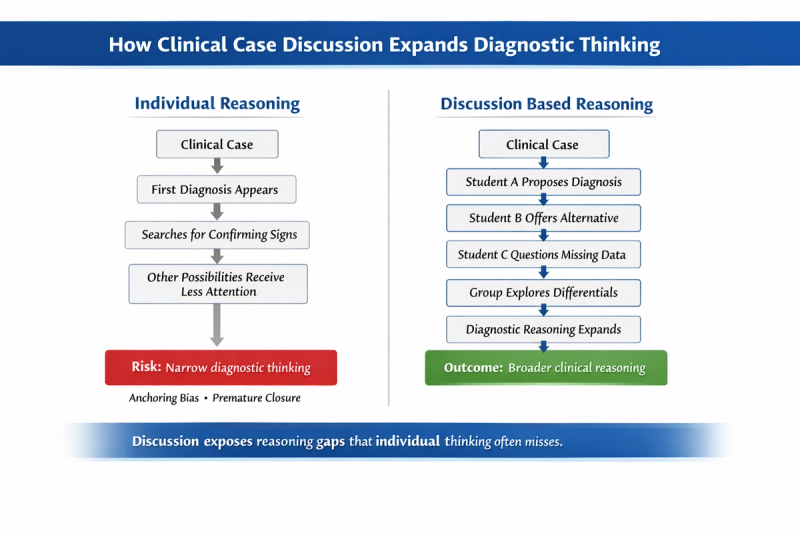
What Happens When Diagnostic Thinking Is Done Alone
When students approach clinical cases alone, their reasoning often follows a narrow path.
The first diagnosis that comes to mind quickly becomes the focus. The student then begins looking for findings that support that idea. Other possibilities receive less attention or are dismissed too early.
Two common reasoning patterns often appear in this situation.
Confirmation bias occurs when a student unconsciously favors information that supports the initial diagnosis while ignoring details that challenge it. For example, a case that resembles myocardial infarction may lead a student to focus heavily on chest pain while overlooking atypical features that suggest another condition.
Premature closure happens when a diagnosis is accepted before alternative explanations are fully explored. Once the mind settles on a conclusion, the diagnostic process often stops.
Another limitation of solitary reasoning is limited exposure to alternative diagnostic thinking paths. A student may reach the correct diagnosis but still miss other reasonable differential diagnoses that peers might have considered.
Over time, this pattern can create the illusion of confidence without strengthening the depth of clinical reasoning.
How Case Discussion Changes the Way Students Think
Clinical case discussions create a different learning environment for diagnostic thinking. Instead of one reasoning path, several perspectives emerge at the same time.
When multiple students analyze the same case, each person brings different knowledge, experiences, and interpretations. One student may focus on risk factors, another on pathophysiology, while someone else may question missing clinical details.
This exposure to multiple diagnostic reasoning paths helps students understand that diagnosis is rarely a single linear process. It is often a comparison of possibilities, supported by evidence and refined through questioning.
Discussions also support pattern recognition through conversation. When students explain why they suspect a particular condition, others begin to connect symptoms, mechanisms, and investigations more clearly.
Equally important is the ability to question assumptions. Peers may ask simple but powerful questions:
- What diagnosis could also explain these symptoms?
- Which finding does not fit the current explanation?
- What investigation would help narrow the differential?
These questions force the group to reconsider the case from different angles. In doing so, diagnostic reasoning becomes more deliberate, reflective, and accurate.
Over time, regular case discussion helps students move from simply choosing answers to actively analyzing clinical problems, which is the foundation of strong diagnostic thinking.
How Clinical Case Discussions Improve Diagnostic Thinking
Clinical case discussions strengthen diagnostic thinking by making the reasoning process visible. It is about understanding how different possibilities are considered, tested against evidence, and gradually refined.
When students work through clinical cases alone, the reasoning process often remains internal. The student may reach a correct conclusion but still miss alternative interpretations or reasoning steps that could strengthen their understanding.
Clinical case discussions change this dynamic. When diagnostic thinking is shared with peers, reasoning becomes visible. Different interpretations emerge, assumptions are questioned, and the group collectively examines how the diagnosis is reached.
Over time, this process strengthens several important aspects of diagnostic thinking.
Exposure to Multiple Diagnostic Hypotheses
One of the most immediate benefits of case discussion is exposure to a broader range of diagnostic possibilities.
When a clinical case is discussed in a group, different students often focus on different aspects of the presentation. One student may recognize a key symptom, another may emphasize a risk factor, while someone else may recall a condition that presents in a similar way.
As a result, the group generates a wider set of differential diagnoses, strengthening differential diagnosis thinking.
This process exposes students to:
- diagnostic possibilities they had not initially considered
- alternative ways of interpreting the same clinical findings
- reasoning strategies used by their peers
Even when the final diagnosis remains the same, the discussion helps students understand how multiple hypotheses are evaluated before narrowing the differential.
Identifying Gaps in Clinical Reasoning
Clinical case discussions also help students recognize gaps in their own reasoning.
When students explain their thought process aloud, peers often notice details that were overlooked or assumptions that were made too quickly. A symptom may not fully fit the proposed diagnosis, or an important clinical feature may not have been considered.
Through discussion, the group may identify:
- missing clinical features that require further clarification
- overlooked red flags that could suggest a more serious condition
- an incomplete differential diagnosis that needs expansion
These moments often become the most valuable learning points in clinical case discussion. Instead of simply correcting the answer, the discussion reveals why a reasoning step was incomplete and how it can be improved.
Over time, students become more attentive to these gaps even when approaching cases independently.
Learning Through Peer Reasoning
Clinical medicine is inherently collaborative. In clinical practice, diagnoses are frequently discussed during ward rounds, case conferences, and multidisciplinary meetings.
Clinical case discussions during training mirror this collaborative environment.
When students explain their reasoning to peers, they must organize their thoughts clearly, justify their interpretations, and respond to questions from others. This process strengthens both analytical thinking and communication skills.
Peer reasoning also exposes students to different approaches to the same clinical problem. One student may think in terms of pathophysiology, another may prioritize epidemiology or risk factors, while another may focus on investigation results.
By observing how others analyze the case, students gradually build a more flexible and comprehensive diagnostic approach.
Through repeated discussions, clinical reasoning becomes less about arriving quickly at a diagnosis and more about carefully evaluating possibilities and refining conclusions, which is a key habit in responsible medical practice.
Why Medical Students Often Lack Spaces for Case Discussion
Clinical case discussions can significantly improve diagnostic thinking for medical students, but many medical students rarely experience them consistently during training.
In theory, clinical education encourages discussion. Case presentations, ward rounds, and bedside teaching are all meant to expose students to shared reasoning. In practice, however, opportunities for students to actively discuss cases are often limited.
As a result, many students continue to study cases individually even though collaborative reasoning would strengthen their clinical thinking.
Two common factors contribute to this gap.
Ward Discussions Are Often Time Limited
Clinical environments are designed primarily for patient care, not for extended student discussions.
During ward rounds, consultants and residents must manage multiple responsibilities such as patient evaluation, treatment decisions, and coordination of care. Teaching moments may occur, but they are usually brief and focused on immediate clinical priorities.
For medical students, this often means that discussions happen quickly or remain centered on the consultant's explanation rather than on the students' reasoning process.
Several practical constraints contribute to this pattern:
- Busy clinical postings, where time pressures limit extended case analysis
- Consultant focused teaching, where senior clinicians explain conclusions rather than exploring student reasoning
- Limited student participation, especially when large groups are present during ward rounds
Because of these constraints, many students leave clinical postings having observed clinical decision making but without having had the opportunity to fully articulate their own diagnostic thinking.
Many Online Forums Lack Structured Clinical Discussion
Because of this gap, many medical students turn to online spaces to discuss cases, clarify doubts, or compare reasoning with peers.
Students frequently search for spaces that function as a medical student discussion forum, hoping to find communities where clinical cases can be analyzed collaboratively. However, many existing platforms are not designed specifically for structured clinical reasoning.
Common limitations include:
- unmoderated discussions, where information quality varies widely
- conversations that are not focused on clinical cases, but on exam tips or general study advice
- scattered threads, where discussions move quickly across unrelated topics
These environments can make it difficult for students to engage in meaningful diagnostic conversations or follow a structured case discussion from presentation to reasoning.
Some platforms are attempting to create dedicated spaces that function more like medical student discussion forumsdesigned specifically for clinical reasoning conversations, where cases can be explored through peer perspectives rather than quick answer exchanges.
For students interested in understanding how these spaces work and what features support productive discussion, the article Medical Student Discussion Forum explores this topic in greater detail.
Why Group Discussion Improves Clinical Learning in Medical Education
Clinical case discussions are one example of a broader learning method widely used in medical education: group discussion.
Medicine is rarely practiced in isolation. Clinical decisions often involve conversations between physicians, residents, nurses, and other specialists. Because of this, medical education has long emphasized collaborative learning approaches such as small group discussions, case based learning sessions, and problem based learning.
When students analyze clinical problems together, the learning process becomes more active and reflective. Instead of simply receiving information, students must explain how they interpret clinical findings and justify their conclusions.
This shared reasoning process helps strengthen both understanding and diagnostic thinking.
Discussion Encourages Active Clinical Learning
Group discussions require students to participate actively in the learning process.
Rather than selecting an answer silently, students must explain their reasoning and respond to questions from peers. This process pushes them to organize their thoughts more clearly and examine the evidence supporting their conclusions.
During a case discussion, students often need to:
- explain the reasoning behind a proposed diagnosis
- defend their differential diagnoses when challenged
- respond to peer questions about symptoms, investigations, or risk factors
This active engagement in clinical case discussions helps students move beyond memorizing information and begin applying clinical knowledge to real patient scenarios.
Shared Reasoning Improves Diagnostic Accuracy
Collaborative discussion can also improve the quality of diagnostic reasoning.
Research in medical education has shown that collaborative learning and problem based discussion can improve understanding and clinical reasoning skills among medical students. Studies examining problem based learning environments have reported stronger knowledge retention and improved clinical reasoning compared with purely lecture based teaching.
One explanation is that group discussions expose students to multiple ways of interpreting the same clinical information. When different perspectives are considered together, the group is more likely to identify alternative diagnoses, question assumptions, and refine the diagnostic approach.
As a result, the final interpretation of the case often becomes more balanced and evidence based.
Peer Discussion Builds Confidence in Clinical Thinking
Another important outcome of group discussion is increased confidence in clinical reasoning.
Many medical students hesitate to express diagnostic ideas during ward rounds or formal teaching sessions. Regular peer discussions provide a safer environment where students can practice explaining their thought process and testing their interpretations.
Over time, students become more comfortable with:
- explaining why a particular diagnosis is likely
- presenting clinical cases in a structured way
- questioning interpretations proposed by others
These skills are essential for effective participation in clinical teams.
The broader benefits of group discussion in medical education extend beyond exam preparation and directly influence how students approach diagnostic reasoning. The cluster article Benefits of Group Discussion in Medical Education explores these learning advantages in more detail.
What a Good Clinical Case Discussion Should Look Like
A well structured clinical case discussion usually follows a clear reasoning sequence. Not every discussion automatically improves diagnostic thinking. For a case discussion to be useful, it needs a clear structure that encourages reasoning rather than quick answers.
A good discussion focuses on how the diagnosis is approached, allowing students to examine clinical information step by step and compare different interpretations before reaching a conclusion.
Start With the Clinical Presentation
A productive discussion begins with the basic clinical scenario.
For example:
A 52 year old male presents with chest pain and sweating.
At this stage, students should focus only on the information provided and begin suggesting possible differential diagnoses. The goal is to generate initial hypotheses before additional data or the final answer is revealed.
This encourages students to think broadly about possible causes rather than immediately searching for confirmation.
Explore Diagnostic Reasoning Step by Step
Once initial differentials are proposed, the group can begin analyzing the case more systematically.
Students examine key elements such as:
- presenting symptoms
- relevant risk factors
- available investigations
- how each finding supports or challenges the differential diagnoses
As the discussion progresses, the group gradually narrows the differential list and identifies the most likely explanation.
This step by step exploration helps students understand how clinical information influences diagnostic decisions.
Focus on Reasoning, Not Just the Final Diagnosis
The value of a case discussion does not come from simply identifying the correct diagnosis. It comes from understanding how the reasoning process unfolded.
A useful discussion reflects on questions such as:
- Why was one diagnosis considered more likely than others?
- Which findings helped narrow the differential?
- Were any important possibilities overlooked initially?
By focusing on reasoning rather than just the answer, students develop a deeper and more reliable approach to clinical problem solving.
How Structured Case Discussion Platforms Can Support Medical Students
While clinical case discussions are valuable for developing diagnostic thinking, students often struggle to find consistent opportunities for these conversations during clinical training.
Digital platforms can help address this gap by creating spaces where clinical cases can be discussed beyond the time constraints of ward rounds or classroom sessions. When designed well, these platforms allow students to examine cases more carefully, compare interpretations, and learn from the reasoning of peers.
Digital Platforms Allow Ongoing Clinical Discussion
Online discussion platforms make it possible for students to continue clinical conversations outside formal teaching environments.
Students can analyze cases:
- outside ward hours, when there is more time for reflection
- across institutions, gaining perspectives from peers in different training environments
- with diverse viewpoints, which often expands the range of diagnostic possibilities considered
This extended interaction allows discussions to develop more gradually and thoughtfully than time limited clinical teaching sessions.
Structured Case Threads Improve Learning
The quality of discussion depends heavily on how conversations are organized.
In many casual forums, discussions move quickly across unrelated topics, making it difficult to follow the reasoning behind a case. Structured case threads create a more focused learning environment.
Typically, they involve:
- one clearly presented case
- multiple diagnostic perspectives from participants
- discussion that follows the reasoning process step by step
This structure helps students trace how different hypotheses are proposed, challenged, and refined during the discussion.
Example: Peer Clinical Discussion Platforms
Some digital platforms are beginning to create dedicated environments for this type of structured discussion. Rather than functioning as general student forums, these spaces focus specifically on clinical cases and diagnostic reasoning.
For example, platforms such as MedCoterie aim to support structured clinical case discussions where medical students can explore diagnostic thinking through peer perspectives and shared reasoning.
Building a Habit of Clinical Case Discussion
Clinical reasoning develops gradually through repeated exposure to clinical cases and diagnostic decisions. While individual study remains important, regularly discussing clinical cases with peers can strengthen the way students analyze symptoms, consider alternatives, and refine their conclusions.
Over time, consistent discussion helps transform case analysis from an exam oriented exercise into a deeper habit of clinical thinking.
Discuss at Least One Case Regularly
Even brief case discussions can improve diagnostic reasoning when practiced consistently.
Reviewing a single case with peers, whether during study sessions or online discussions, encourages students to pause and examine the reasoning behind possible diagnoses rather than simply identifying the final answer.
Regular exposure to different cases gradually expands clinical pattern recognition and strengthens the ability to approach unfamiliar presentations.
Ask What Other Diagnoses Could Fit
One of the most useful habits in case discussion is deliberately exploring alternative diagnoses.
After proposing a likely diagnosis, students can ask simple but important questions such as:
- What other conditions could explain these symptoms?
- Which findings do not fully match the current explanation?
- What additional information would help narrow the differential?
This practice encourages broader differential diagnosis thinking and reduces the tendency to settle too quickly on a single conclusion.
Treat Discussion as Diagnostic Training
The goal of case discussion is not simply to reach the correct answer but to strengthen the reasoning process behind clinical decisions.
When students treat discussions as an opportunity to examine how diagnoses are formed, each conversation becomes a form of diagnostic training. Over time, this habit builds a more careful and reflective approach to clinical problem solving.
Consistent discussion, even in small groups or informal settings, can therefore play an important role in developing confident and thoughtful clinical reasoning.
References :
Schmidt HG, Rotgans JI, Yew EHJ.
The process of problem-based learning: What works and why.
Medical Education. 2011;45(8):792–806.
https://pubmed.ncbi.nlm.nih.gov/21752076/
Hmelo-Silver CE.
Problem-based learning: What and how do students learn?
Educational Psychology Review. 2004;16(3):235–266.
https://doi.org/10.1023/B:EDPR.0000034022.16470.f3
Wood DF.
ABC of learning and teaching in medicine: Problem based learning.
BMJ. 2003;326(7384):328–330.
https://doi.org/10.1136/bmj.326.7384.328
Jin J, Bridges SM.
Educational technologies in problem-based learning in health sciences education: A systematic review.
Journal of Medical Internet Research. 2014;16(12):e251.
https://www.jmir.org/2014/12/e251/