Anchoring Bias in Diagnosis: Real Clinical Examples for Medical Students

You read the first two lines of the case and your brain already knows the answer.
Young patient. Fever. Productive cough. Pneumonia.
You start building your reasoning around it. You stop searching for alternatives. Every new symptom either fits your diagnosis or gets quietly ignored.
That moment is anchoring bias in diagnosis.
Most of us have done this during case discussions or while practicing alone. We feel relieved that something looks familiar, and we move quickly toward closure. As medical students, we are still learning how to hold uncertainty. The first answer that feels right often feels relieving.
The problem is that anchoring bias does not feel like an error. It feels like clarity. And that is exactly why it is dangerous.
What Is Anchoring Bias in Diagnosis?
Anchoring bias in diagnosis happens when you fixate on the first clinical impression and allow it to guide the rest of your reasoning.
It usually begins with something that feels familiar. A keyword in the history. A classic symptom. A pattern you recently revised. Once that initial diagnosis forms, your brain starts organizing everything around it. Supporting findings feel important. Contradictory findings feel less significant.
The issue is not that early hypotheses are wrong. In fact, experienced clinicians often use early pattern recognition effectively. The problem arises when the first impression goes unchallenged. When we stop actively asking, “What else could this be?”
For medical students, anchoring bias often appears during case presentations and viva practice. We want to show that we recognize common diagnoses quickly. Speed feels like competence. But clinical reasoning is not just recognition. It requires deliberate verification before closure.
How Anchoring Bias Happens During Clinical Reasoning
Clinical reasoning often begins with pattern recognition. You hear a few key symptoms and your mind quickly matches them to a condition you have studied before. That early hypothesis is not the problem. It is a normal cognitive shortcut.
Anchoring bias begins when that hypothesis becomes fixed too early.
Instead of generating multiple differentials, you start collecting evidence only for the first diagnosis. Lab results are interpreted through that lens. History points that do not fit are explained away rather than explored. You may not even realize this is happening. It feels like efficient thinking.
In reality, the reasoning process has narrowed before it was fully opened.
Why Medical Students Are Particularly Vulnerable
Medical students are still developing diagnostic depth. Because of that, every recognizable presentation feels rewarding. Identifying something quickly gives a sense of progress and competence.
There is also subtle pressure during case discussions. When you present a confident diagnosis early, it feels strong. Pausing to say, “I am still considering alternatives,” can feel like uncertainty.
But early confidence without structured evaluation increases the risk of premature closure. Unlike experienced clinicians who have seen variations of the same disease repeatedly, students often rely on limited exposure. That makes the first familiar explanation more persuasive than it should be.
Anchoring bias does not happen because students are careless. It happens because learning medicine trains us to recognize patterns before we are fully trained to challenge them.
A Real Clinical Scenario: How Anchoring Bias Leads to the Wrong Diagnosis
The Initial Presentation
A 52 year old man presents with central chest pain for two hours. The pain is burning in character and started after a heavy meal. He has a history of hypertension. His ECG is normal. Vitals are stable.
During case discussion, the first thought that comes up is gastritis or acid reflux. The pain began after food. It is described as burning. The ECG does not show acute changes.
That initial label feels reasonable.
The First Diagnostic Anchor
Once “gastritis” enters the discussion, the reasoning begins to narrow.
The burning nature of pain is emphasized. The recent heavy meal becomes the central clue. The normal ECG provides reassurance. The absence of dramatic instability makes the case feel low risk.
No one pauses to ask whether the history is fully consistent. No one lists serious alternatives out loud.
The diagnosis has anchored.
What Was Missed
The patient is 52. He has hypertension. The pain is central, not clearly epigastric. It has lasted two hours without relief.
Cardiac enzymes were not considered initially because the first explanation felt sufficient. The possibility of an atypical presentation of acute coronary syndrome was not actively explored.
Nothing was hidden. The clues were present. They were filtered through the first impression.
What Changed the Diagnosis
A senior clinician reviewing the case asks a simple question:
“What if this is not gastritis?”
Troponin levels are ordered. They return elevated. The diagnosis shifts to non ST elevation myocardial infarction.
The initial reasoning was not irrational. It was incomplete.
Anchoring bias did not occur because the students lacked knowledge. It occurred because the first plausible answer reduced the motivation to continue searching.
Why Anchoring Bias Is Dangerous in Early Clinical Training
Anchoring bias becomes particularly significant during early clinical years because this is when reasoning habits are formed. The way you approach cases now often becomes the default method you carry into internship and beyond.
The danger is not just a missed diagnosis. It is reinforcing a reasoning habit that closes too early.
Premature Closure in Case Discussions
Premature closure happens when the diagnostic process stops after the first reasonable answer.
In classroom discussions, this may look like presenting one diagnosis confidently and moving straight to management. Alternative possibilities are not explored, not because they are impossible, but because the discussion feels “complete.”
Over time, this trains the brain to associate speed with competence. The habit of systematically expanding differentials weakens. That subtle shift in reasoning style is where anchoring bias becomes entrenched.
Overconfidence After Pattern Recognition
Recognizing patterns is an important clinical skill. The problem begins when recognition replaces verification.
When you correctly identify a few classic cases, confidence increases. That confidence is valuable. But it can also reduce the perceived need to double check assumptions.
In early training, exposure is still limited. A student may have seen three textbook presentations of a condition and begin to believe they fully understand it. Variations and atypical cases are underestimated.
Anchoring bias often grows quietly from that early confidence.
The Illusion of “Knowing the Topic”
There is also a psychological layer to this.
After revising a system thoroughly, it feels familiar. During the next case discussion on that topic, the brain searches for something that matches the recently studied material. When it finds a partial match, it feels satisfying.
That satisfaction can create an illusion of mastery. Instead of asking, “What else fits better?” the reasoning process focuses on reinforcing what is already known.
This is not about intelligence or effort. It is about how the mind naturally seeks coherence and certainty.
In early clinical training, learning to tolerate uncertainty is just as important as learning to recognize patterns.
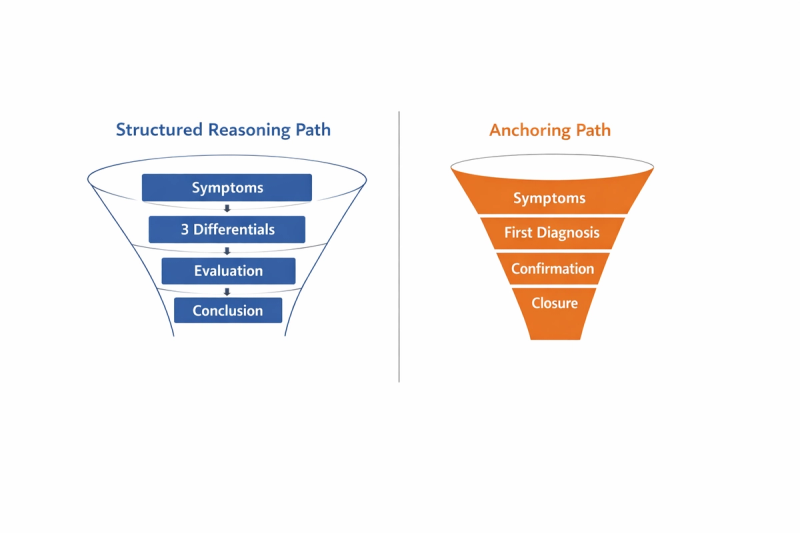
How to Break Anchoring Bias During Daily Case Practice
The goal is not to eliminate your first impression. It is to prevent it from becoming final too early.
Anchoring bias becomes weaker when your reasoning process is structured instead of reactive. Small habits during daily case practice can reduce diagnostic narrowing.
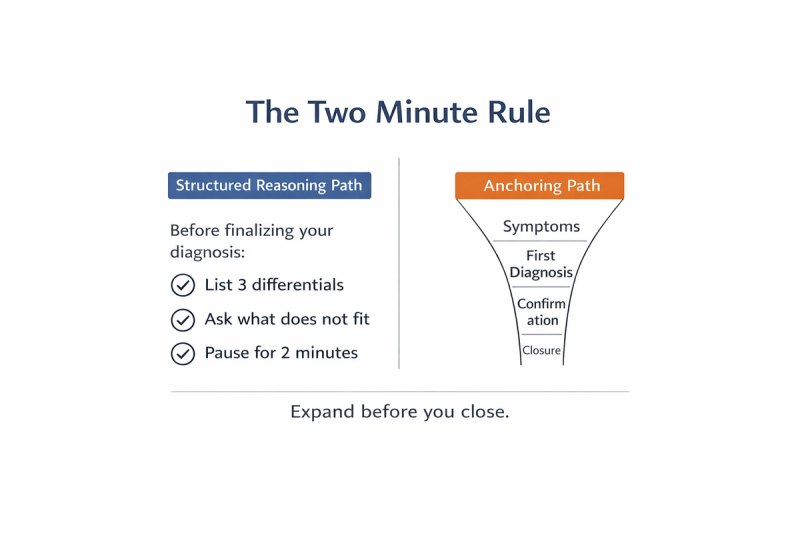
Force Yourself to List Three Differentials
Even if the first diagnosis feels obvious, pause and write down at least three plausible alternatives.
They do not all need to be equally likely. The purpose is to widen your thinking before narrowing it again. When you deliberately generate alternatives, you interrupt automatic anchoring.
Over time, this becomes easier. The brain learns that every case deserves expansion before closure.
Ask “What Does Not Fit?”
After forming your initial diagnosis, actively search for one feature that does not align perfectly.
Is there a symptom that feels slightly inconsistent?
Is the timeline unusual?
Is a risk factor missing?
This single question shifts you from confirmation mode to evaluation mode. Anchoring bias thrives when we look only for supporting evidence. It weakens when we look for contradiction.
Delay Diagnostic Closure by Two Minutes
During self practice or group discussion, avoid concluding immediately.
Give yourself two deliberate minutes after forming the first diagnosis. Use that time to review the history again and reconsider alternatives. This short pause may feel unnecessary, but it builds cognitive discipline.
Clinical reasoning is not a race. In training, depth matters more than speed.
Use Structured Case Frameworks
Unstructured thinking increases cognitive bias. A consistent framework reduces it.
When you approach cases systematically, through history review, differential expansion, justification, and reflection, you create checkpoints that prevent early closure. Structure forces your reasoning to stay open longer than your first instinct.
This is why daily structured practice matters. If you build a habit around a simple, time bound reasoning routine, such as the approach outlined in How to Practice Clinical Cases Daily as a Medical Student: A Structured 15-Minute Framework, anchoring becomes less likely without requiring constant self correction.. The structure itself slows premature certainty.
Peer discussion strengthens this further. In reflective case spaces like MedCoterie, where reasoning is shared rather than simply declared, alternative differentials surface more naturally. When someone asks, “What else could this be?” it exposes anchoring patterns that are harder to detect alone.
Anchoring bias weakens when your thinking is both structured and visible.
A Simple Cognitive Habit That Prevents Anchoring Bias
Before you finalize any diagnosis during practice, ask yourself one deliberate question:
“If I am wrong, what else could this be?”
That single pause creates space between your first impression and your final conclusion. It shifts your brain from confirmation to evaluation.
You do not need to distrust your instincts. You need to test them.
Clinical reasoning improves not when you think faster, but when you think wider before you think narrower.
If you build the habit of expanding before closing, anchoring bias becomes easier to recognize. And over time, that small cognitive discipline becomes part of how you think, not something you force yourself to remember.
References
- Croskerry P. The importance of cognitive errors in diagnosis and strategies to minimize them. Academic Medicine. 2003;78(8):775–780.
- Croskerry P. Diagnostic failure: A cognitive and affective approach. In: Advances in Patient Safety: From Research to Implementation. Vol 2. Rockville, MD: Agency for Healthcare Research and Quality; 2005.
- Graber ML, Franklin N, Gordon R. Diagnostic error in internal medicine. Archives of Internal Medicine. 2005;165(13):1493–1499.
- National Academies of Sciences, Engineering, and Medicine. Improving Diagnosis in Health Care. Washington, DC: The National Academies Press; 2015.
- Norman G, Monteiro S, Sherbino J. Is clinical cognition binary or continuous? Advances in Health Sciences Education. 2013;18(3):435–446.